(Acute Pericarditis video – Click to skip to video)
Acute Pericarditis is the acute inflammation of the Pericardium.
Causes
- Viral (common cause) – Coxsackie B, Echovirus
- Uremia
- Tuberculous pericarditis
- Connective tissue diseases – SLE, Scleroderma
- Post-Myocardial Infarction – on 2nd or 3rd day or in Dressler’s syndrome
- Bacterial infections – Staph aureus, H. influenzae
- Acute Rheumatic Fever
- Malignancy – From carcinoma of bronchus, breast; lymphoma, leukaemia
- Drugs – Doxorubicin, Cyclophosphamide
- Radiation
- Fungal – Histoplasmosis, Coccidioidomycosis
Symptoms
- The main symptom is chest pain which is retrosternal, sharp or stabbing in nature, may radiate to the shoulder and neck.
- Aggravated by movement, lying down, deep breathing, exercise & swallowing.
- Pain is relieved by sitting or bending forward.
- Symptoms related to the diseases causing pericarditis (e.g. low-grade evening rise of temperature, night sweat weight loss in TB).
Signs
The prominent sign of Pericarditis is pericardial friction rub which is produced due to rubbing of inflamed & roughened visceral & parietal pericardial surfaces against each other. Its characteristics are as follows:
- It is a high-pitched, harsh, scratching, grating, leathery sound, to and fro in quality.
- Better heard over the left lower parasternal region with the patient leaning forward.
- Augmented by pressing the stethoscope.
- Usually heard in systole, but maybe in diastole.
- Present even after holding the breath (to differentiate from pleural rub).
Investigations
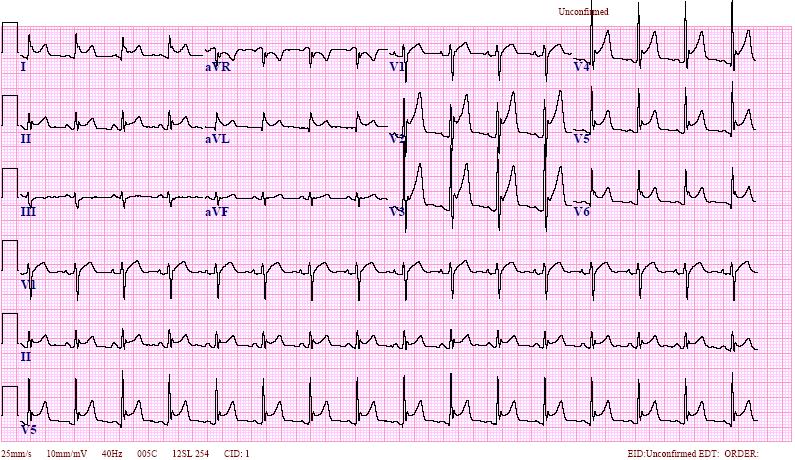
ECG – ST-elevated with an upward concavity in most of the leads (Saddle-shaped)
Chest X-ray – usually normal but may show effusion and other features of associated diseases in chest.
Echocardiography – A valuable tool to exclude pericardial effusion and to see cardiac structure & function.
Other tests—To look for causative disease
Treatment
- Symptomatic Treatment
- Analgesia – NSAIDs (Indomethacin or Ibuprofen)
- In severe or recurrent pain—Corticosteroids may be tried but they do not accelerate the cure
- If no response to steroid—Azathioprine or Colchicine may be added
- If recurrence with no response to medical treatment—Pericardiotomy may be done
- Treatment of Primary cause. e.g., antibiotic for a bacterial infection or Anti-TB treatment, if tuberculosis is diagnosed.