The Ashman phenomenon is also known as Ashman beat or Ashman aberrancy.
This phenomenon is mainly of academic interest because it is clinically not symptomatic on its own and there is no treatment.
Background
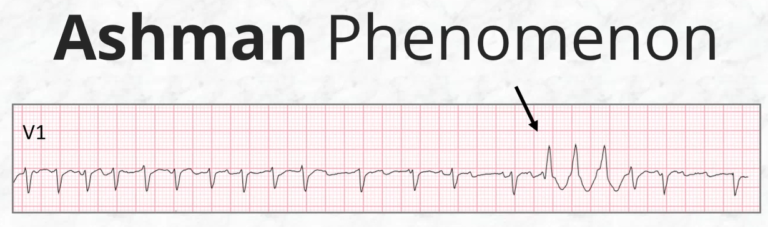
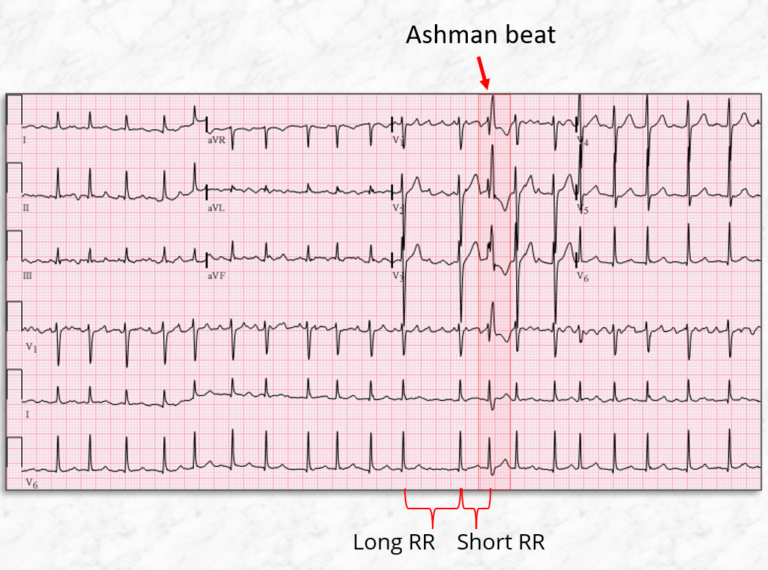
This phenomenon was described by Gouaux and Ashman, in 1947, in patients with atrial fibrillation. It was detected that a relatively long cardiac cycle or R-R interval in ECG was followed by a relatively short cycle or R-R interval, the QRS complex with a short cycle often has Right Bundle Branch Block (RBBB) morphology.
Mechanism
The refractory period of the His-Purkinje system is proportional to the R-R interval of the preceding beat. When there is a long R-R interval, the subsequent refractory period will be relatively long. During this long refractory period, if a premature supraventricular stimulus occurs (as is expected in cases of AF), whilst the His-Purkinje system is still refractory, then the conducted beat will appear abnormal. Because the refractory period of the right bundle is slightly longer than the left bundle, the aberrantly-conducted beat travels through the left bundle first and typically demonstrates a right bundle branch block morphology.
Criteria for Ashman Phenomenon
Fisch criteria are used for the diagnosis of the Ashman phenomenon. It includes these 5 points.
1. The cycle terminated by the aberrant QRS complex is preceded by a relatively long cycle.
2. Right bundle branch block aberrancy with a normal orientation of the initial QRS vector is seen. A series of wide QRS supraventricular beats are possible.
3. Irregular coupling of aberrant QRS complexes i.e., the Ashman beats occurs at irregular intervals.
4. A short-long-short RR interval is even more likely to initiate aberration.
5. Lack of fully compensatory pause.
Post finishes here. Please watch this brief video to revise what you have learned