Bronchiectasis is a common case scenario in written exams, OSCEs, as well as in clinical practice. We have published a YouTube video and Q&A post on this important topic, but in this post, we will only give you the best tips regarding bronchiectasis.
HRCT chest demonstrating bronchiectasis
1. Definition
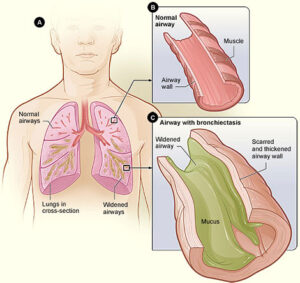
Bronchiectasis is abnormal, permanent dilatation of bronchi and bronchioles (proximal to respiratory bronchioles). It can result from either congenital or acquired causes.
2. Pathophysiology
Congenital or acquired causes, lead to chronic inflammation of the bronchi and bronchioles resulting in dilatation and thinning of these airways.
Once bronchiectasis develops, patients have chronic suppurative airway infection with copious sputum production. There is progressive scarring of the affected areas and lung damage occurs.
The commonest characteristic symptom of bronchiectasis is a chronic cough with copious purulent sputum.
6. Characteristic signs in bronchiectasis
Fingernail clubbing.
Mid-inspiratory coarse moist crackles over the affected area on auscultation. Crackles vanish or changes in character after cough.
7. Complications
– Infective exacerbations )most commonly encountered complication) – Pneumonia – Massive hemoptysis – Lobar/lung collapse – due to airway blockade by tenacious sputum – Amyloidosis – Lung abscess/empyema
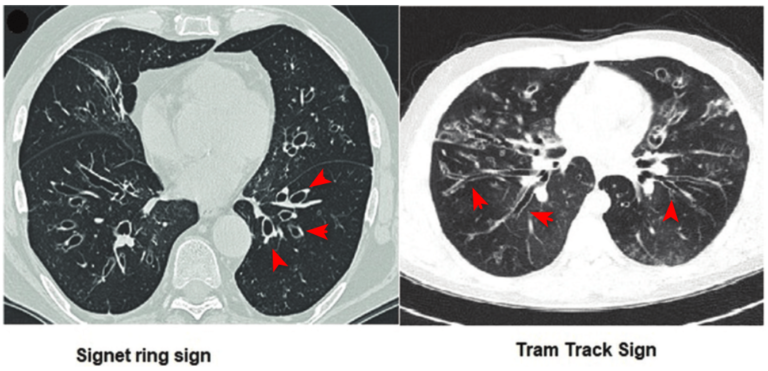
8. High-resolution CT scan is sensitive and diagnostic test of choice
Characteristic findings on HRCT scan chest are Tram-track appearance and signet ring shadows, representing dilated bronchi, longitudinally and in cross-section, respectively.
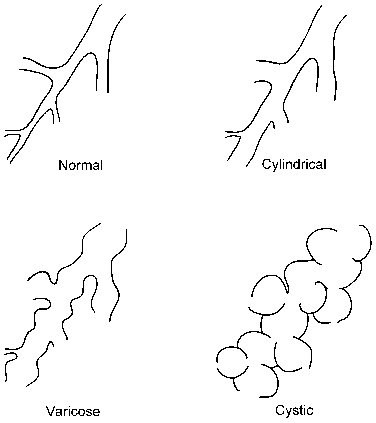
9. There are 3 types of bronchiectasis based on shape of dilated bronchi on CT scan
1. Cylindrical or tubular, 2. Varicose, and 3. Cystic. Tubular bronchiectasis is the most common one.
10. Based on extent, bronchiectasis is divided into 2 types of bronchiectasis
Bronchiectasis can also be categorized based on the extent, into focal and diffuse. 1. Focal bronchiectasis indicates local pathology, like bronchiectasis due to a foreign body, due to intrabronchial tumor, or compressing from outside. 2. Diffuse bronchiectasis indicates systemic disease.
11. Fibrotic lung diseases can lead to bronchiectasis without infection
This is known as ‘Traction bronchiectasis.’ In fibrotic lung diseases or post-TB lung fibrosis, there is a pull or traction on the bronchi arising from parenchymal distortion. This leads to the dilatation of these airways.
12. Location of bronchiectasis can give you clues regarding etiology!
Bronchiectasis location can give clues regarding the cause. – Central bronchiectasis – occurs in ABPA. – Upper lung fields – occurs in cystic fibrosis and post-radiation lung fibrosis. – Middle lung fields – occurs in nontuberculous mycobacterial infections. – Lower zones – occurs in recurrent aspiration pneumonia (e.g., in scleroderma-associated esophageal dysmotility), traction bronchiectasis secondary to interstitial lung diseases, or recurrent immunodeficiency related lung infections e.g., hypogammaglobulinemia.
13. Main management principle is effective sputum expectoration
– Efficient airway clearance helps a lot in improving quality of life, and also prevents infective exacerbations and other complications. – Chest physiotherapy, postural drainage techniques, the use of flutter valve devices, and the use of mucolytic agents all help in sputum expectoration and clearance of the airways.
14. Increase in sputum quantity and purulence is indicative of acute infective exacerbation of bronchiectasis
This may occurs even in the absence of fever or appearance of new opacities on radiograph.
15. Treatment of infective exacerbation will help in stopping hemoptysis in most of the cases
Only occasionally, you may require pulmonary artery embolization in massive/life-threatening hemoptysis.
16. Patient will require prophylactic antibiotics if there are 3 or more infective exacerbations of bronchiectasis per year.
Consider prophylaxis for such patients. There are a number of regimens for this purpose.
17. Vaccination
Bronchiectasis patients shall receive pneumococcal and annual influenza vaccines.