Introduction
Deep vein thrombosis (DVT) is the manifestation of the disease entity, venous thromboembolism (VTE). Clot formation occurs in the deep veins of the legs or arms. These clots can dislodge and settle in the pulmonary artery causing a pulmonary embolism (PE) which is the second manifestation of VTE. Chronically, the DVT can damage the venous valves leading to venous insufficiency and thus its sequelae.
What are the risk factors for DVT?
- Increased age
- Pregnancy
- Synthetic estrogens
- Surgery (hip or knee surgery, major abdominal or pelvic surgery in cancer patients)
- Trauma
- Past DVT
- Cancer
- Obesity
- Immobility
- Thrombophilia
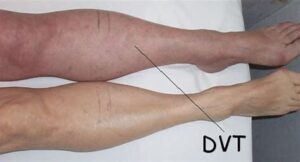
What are the signs of DVT?
- Inflammation of calf region. There will be warmth, tenderness, swelling and erythema.
- Mild fever
- Pitting oedema
What is the differential diagnosis of DVT?
- Cellulitis
- Ruptured Baker’s cyst
- Gastrocnemius muscle tear
- Compartment syndrome
How to prevent DVT?
- Assess all patients for risk of VTE at the time of admission and administration of appropriate prophylaxis if indicated
- Low Molecular Weight Heparin (LMWH) to high-risk patients. Unfractionated heparin if eGFR less than 30mL/min/1.73m2.
- Fondaparinux (a factor Xa inhibitor) decrease the risk of DVT over LMWH in eg major orthopaedic surgery without the increased risk of bleeding.
- Mechanical prophylaxis: Graduated compression stockings and intermittent pneumatic compression devices.
- Stop oral contraceptive pills 4 weeks pre-operatively
- Early mobilization
Approach to the diagnosis of DVT
As a first step, calculate Wells score in suspected DVT cases
| Clinical Features | Score |
|---|---|
|
Active cancer (treatment within last 6 months or palliative) |
1 |
|
Paralysis, paresis, or recent plaster immobilization of leg |
1 |
|
Recently bedridden for > 3 days or major surgery in last 12 weeks |
1 |
|
Local tenderness along distribution of deep venous system |
1 |
|
Entire leg swollen |
1 |
|
Entire leg Calf swelling >3cm compared with asymptomatic leg (measured 10cm below tibial tuberosity) swollen |
1 |
|
Pitting oedema (greater in the symptomatic leg) |
1 |
|
Collateral superficial veins (non-varicose) |
1 |
|
Previously documented DVT |
1 |
|
Alternative diagnosis at least as likely as DVT |
– 2 |
Score 2 or more = DVT likely
– A proximal leg vein ultrasound scan should be carried out within 4 hours
- if the result is positive then a diagnosis of DVT is made and anticoagulant treatment should start
- if the result is negative a D-dimer test should be arranged. A negative scan and negative D-dimer make the diagnosis unlikely and alternative diagnoses should be considered
– If a proximal leg vein ultrasound scan cannot be carried out within 4 hours a D-dimer test should be performed and interim therapeutic anticoagulation administered whilst waiting for the proximal leg vein ultrasound scan (which should be performed within 24 hours)
- interim therapeutic anticoagulation used to mean giving low-molecular-weight heparin
- NICE updated its guidance in 2020. They now recommend using an anticoagulant that can be continued if the result is positive.
- this means normally a direct oral anticoagulant (DOAC) such as apixaban or rivaroxaban
– If the scan is negative but the D-dimer is positive:
- stop interim therapeutic anticoagulation
- offer a repeat proximal leg vein ultrasound scan 6 to 8 days later
Score 1 or less = DVT unlikely
– Perform a D-dimer test
- this should be done within 4 hours. If not, interim therapeutic anticoagulation should be given until the result is available
- if the result is negative then DVT is unlikely and alternative diagnoses should be considered
- if the result is positive then a proximal leg vein ultrasound scan should be carried out within 4 hours
– If a proximal leg vein ultrasound scan cannot be carried out within 4 hours interim therapeutic anticoagulation should be administered whilst waiting for the proximal leg vein ultrasound scan (which should be performed within 24 hours)
What is the treatment of DVT?
– Elevate and immobilize the affected leg to reduce limb oedema.
– Use simple analgesia to relieve pain.
– Mainstay of treatment of VTE/DVT is anticoagulation.
- Direct oral anticoagulants (DOACs): Recent NICE guidelines advocate the use of DOACs, e.g., dabigatran, apixaban, and rivaroxaban in most cases right from the start. These have simpler dosing and monitoring, and there is reduced bleeding risk.
- LMWH or fondaparinux can also be used. LMWH is superior to unfractionated heparin. Unfractionated heparin is used in renal failure or if increased risk of bleeding. Cancer patients should receive LMWH for 6 months and then review. In others, start warfarin simultaneously with LMWH because warfarin is prothrombotic for the first 48 hours. Stop heparin when INR is 2–3. Then continue treatment for 3 months in most and the duration can then be extended in some cases.
- Inferior vena cava filters shall be used to prevent PE in patients with active bleeding or in whom anticoagulation has failed.