Lung auscultation is an integral part of the chest examination. The auscultation findings provide many useful signs that are helpful in establishing a diagnosis.
This post is all about the most common auscultation findings. To help reinforce the theory, there are videos with the audio of these lung sounds
(Please use headphones for the videos)
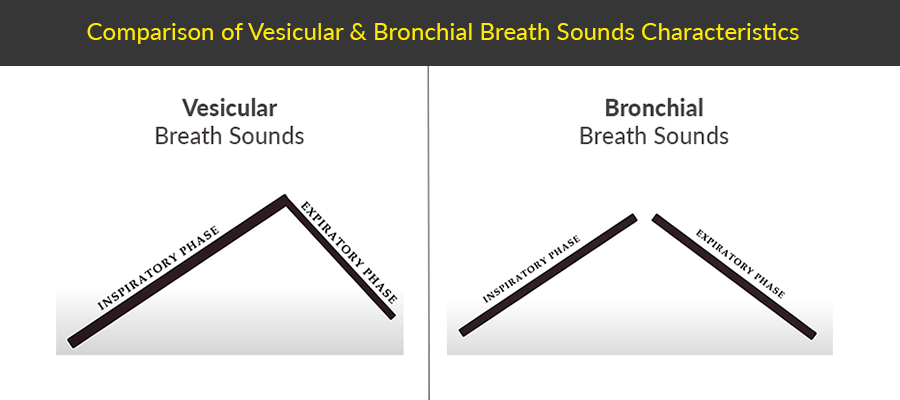
The normal breath sounds are called vesicular. It is a soft, low-pitched sound heard in most parts of the lung fields.
In vesicular sound, the inspiratory phase is longer than the expiration, without any pause between the two phases (see first figure below).
Abnormalities:
Abnormalities in vesicular breath sounds can be of 3 types:
1. You hear Bronchial breath sounds in part of the lungs where there is supposed to be vesicular sound
2. Vesicular breath sounds have become Diminished or Absent, or
3. Some Added/Adventitious breath sounds are also audible in addition to vesicular breath sounds
This oversimplification of types is just for understanding. You may be able to find all three findings simultaneously.
1. Bronchial Breath Sounds
Bronchial breathing is hollow, tubular in quality, and high-pitched quality sound. Unlike vesicular breath sounds, there is a definite gap between the inspiration and expiration phases.
2. Diminished or Absent Breath Sounds
The breath sounds may be less audible or altogether absent in certain conditions, such as pleural effusions, pneumothorax, or emphysema.
3. Added or Adventitious Sounds
Added or Adventitious sounds include:
(i) Wheezes
(ii) Crepitations
(iii) Pleural Friction Rub
(iv) Stridor
Let’s explore these one by one.
(i) Wheezes
Wheezes are whistling quality sounds heard on auscultation, but sometimes can be audible without the help of a stethoscope.
Wheezes are classified as either sibilant wheezes or sonorous wheezes (rhonchi).
They are caused by a partial obstruction in the airways that is commonly either due to secretions or bronchoconstriction.
- Sibilant Wheeze – High-Pitched wheeze
The sibilant wheeze is the wheeze that most healthcare professionals are familiar with as heard in bronchial asthma.
They are characterized by a high-pitched, continuous sound that occurs either at the end of inspiration or during the expiratory phase.
Mechanism: They are caused by the narrowing of airways around obstructions. During inspiration, the elasticity of the airways will cause them to dilate, which will allow air to flow around the obstruction. As the airways contract during exhalation and airflow increases, it produces a high-pitched wheeze. - Sonorous Wheeze (Rhonchi) – Low Pitched
The sonorous wheeze, also commonly referred to as rhonchi, is caused by the same expansion and narrowing of the airways as sibilant wheezes. The difference between the two is that rhonchi are typically associated with secretions that obstruct the larger airways. This causes a lower-pitched vibrating sound on auscultation that is similar to snoring. Because rhonchi are caused by airway secretions, they can usually be heard both during the inspiratory phase and expiratory phases (biphasic).
(ii) Crackles / Crepitations / Rales
Crackles are interrupted and non-musical quality sounds, and are usually Inspiratory. In some diseases, the peripheral airways collapse on expiration due either to interstitial fibrosis or secretions/fluid in the peripheral airways. During inspiration, rapid air entry abruptly opens up these collapsed smaller airways and alveoli, producing a crackling noise.
Crackles can be heard in different phases of respiration, such as:
- Early-Inspiratory in smaller airway diseases like bronchiolitis.
- Mid-Inspiratory in pulmonary edema.
- Late-Inspiratory in pulmonary fibrosis, pulmonary edema, COPD, resolving pneumonia, lung abscess, tuberculous lung cavities.
- Biphasic – as the name indicate, these are heard in both phases of respiration e.g., in bronchiectasis.
The crackles can also be characterized based on their sound quality into Fine & Coarse.
- Fine Crepitations are heard in bronchiolitis, Pulmonary edema, and Pulmonary fibrosis.
- Coarse crepitations are featured in COPD, Resolving pneumonia, Lung abscess, Tuberculous lung cavities, or bronchiectasis.
(iii) Stridor
Stridor is caused by the narrowing/obstruction of larger airways.
Classically speaking, stridor is not an auscultated lung sound, but it is a sound audible without a stethoscope.
(iii) Pleural Rub
A pleural rub is a low-pitched, grating sound similar to the sound of walking on snow, and it is most commonly caused by an inflammation of either visceral and/or parietal pleura(e).
At times, you may want to differentiate pleural rub from pericardial rub. In order to do so, perform a brief inspiratory hold maneuver. If the rub continues during the maneuver, it is most likely a pericardial rub.
Did you find this post useful?
Please share your comments in the comments section.
I?¦ll right away snatch your rss feed as I can not to find your e-mail subscription link or newsletter service. Do you’ve any? Please let me know in order that I could subscribe. Thanks.