History of daytime excessive sleepiness, and snoring at night is typical. Daytime tendency to fall asleep can be assessed quantitatively with a questionnaire, like given below:
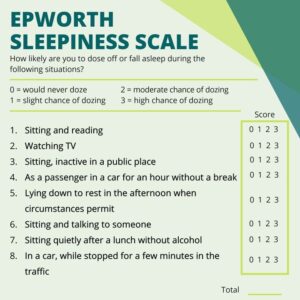
Provided that sleepiness does not result from inadequate sleep time, anyone who repeatedly falls asleep during the day should be referred for a sleep assessment.
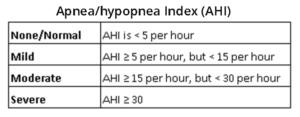
Polysomnography (Overnight studies of breathing, oxygenation, and sleep quality) is diagnostic. The severity of OSAHS is determined by the number of apnoea/hypopnoea per hour of sleep (apnoea/hypopnoea index, AHI).
Apnoea = a 10-second or longer breathing pause
Hypopnoea = a 10-second or longer 50% reduction in ventilation that results in a 4% drop in arterial oxygen saturation.