1- Radiological investigations
(i) Chest X-ray – PA view
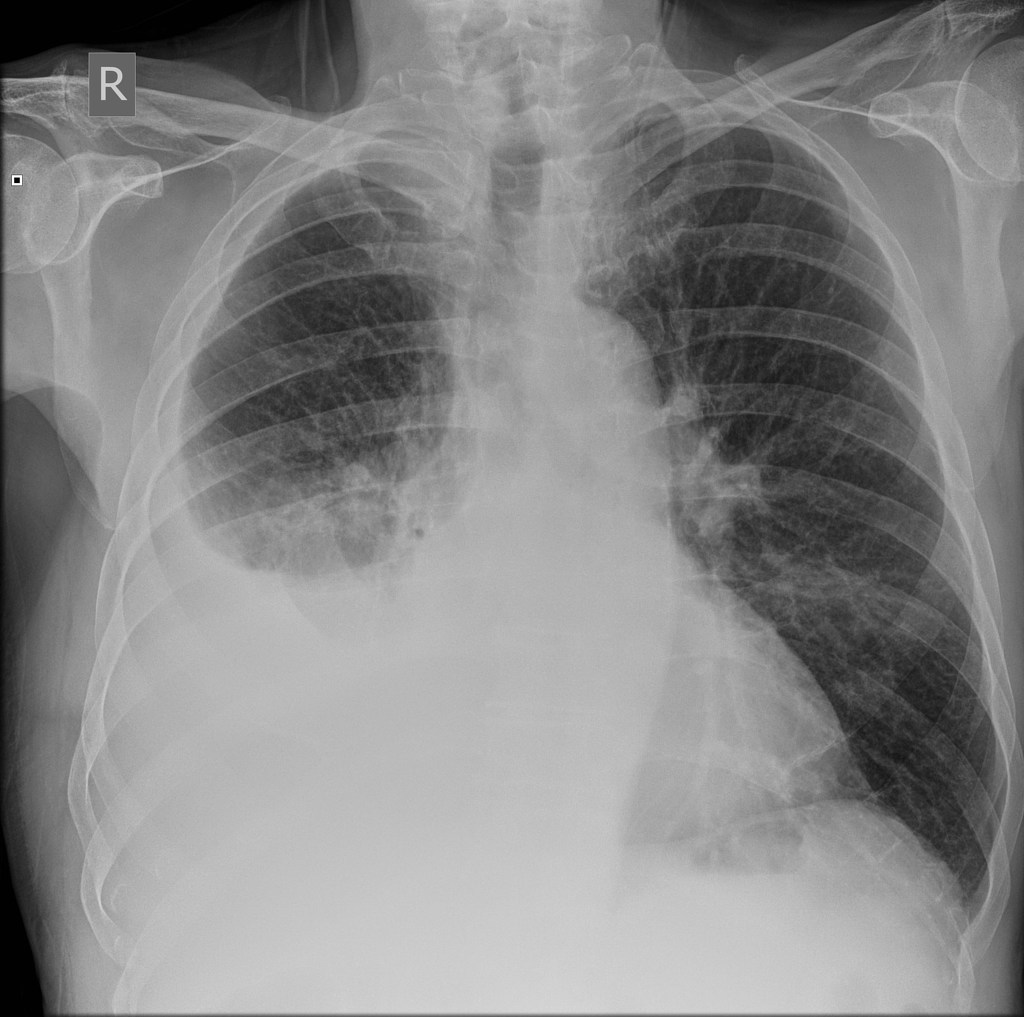
The classical appearance of pleural fluid (on erect PA chest film) is of a curved shadow at the lung base, blunting the costophrenic angle, and the fluid meniscus ascending towards the axilla.
Around 200 mL of fluid is required to be detectable on a PA chest X-ray.
Previous scarring or adhesions in the pleural space can cause localized effusions.
Subpulmonary effusion, which is pleural fluid localized below the lower lobe, simulates an elevated hemidiaphragm.
Pleural fluid localized within an oblique fissure may produce a rounded opacity that may be mistaken for a tumor. This is called pulmonary pseudotumor.
(ii) Ultrasound is more accurate than plain chest X-ray for detecting the presence and then quantification of fluid.
A clear hypoechoic space is consistent with a transudate, and the presence of moving, floating densities suggests an exudate.
The presence of septation most likely indicates an evolving empyema or resolving haemothorax.
(iii) CT scan – It is indicated when a malignant disease underlying the effusion is suspected.
Some really prime content on this web site, bookmarked.
Thanks for the thoughts you are giving on this blog. Another thing I would like to say is that getting hold of duplicates of your credit rating in order to inspect accuracy of each detail would be the first measures you have to accomplish in credit improvement. You are looking to clear your credit profile from destructive details faults that ruin your credit score.
Thanks for sharing.
Great notes on pleural effusion quite accurate and practical. How I wish we demonstrated a technique for therapeutic pleural tap towards the end.
Good idea. Will try to update the post with this. Thank you!